Prostate cancer is the most common diagnosis treated in the proton centers worldwide. It is the diagnosis where the largest number of patients have been treated with protons (tens of thousands). The reason is that prostate cancer is relatively common and the target volume that needs to be irradiated is small. Additionally, the tissues through which the proton beam must pass (muscles and skeleton) is stable thorough treatment. Although prostate cancer is extensively discussed in the professional community and it should be noted that there are currently no randomized studies comparing photon and proton radiotherapy for this diagnosis, the results of many thousands of treated patients speak unambiguously for proton radiotherapy.
Summary of results of published studies relating to prostate carcinoma:
Based on the latest published data, the 5-year survival rate without PSA relapse is 97–99% for low-risk prostate carcinoma, 85–95% for moderate-risk prostate carcinoma, and 75–85% for high-risk prostate carcinoma. Such results are usually achieved using neither photon techniques nor surgical procedures.
Proton radiotherapy has minimal toxicity (side effects). Recently published studies describe severe toxicity of treatment in less than 1% of a large population of patients. When compared with published data on photon radiotherapy and surgeries, such toxicity is minimal and significantly lower than that in other methods.
Unlike surgical therapy, proton therapy does not lead to the development of impotence, thus significantly enhancing patients’ quality of life.
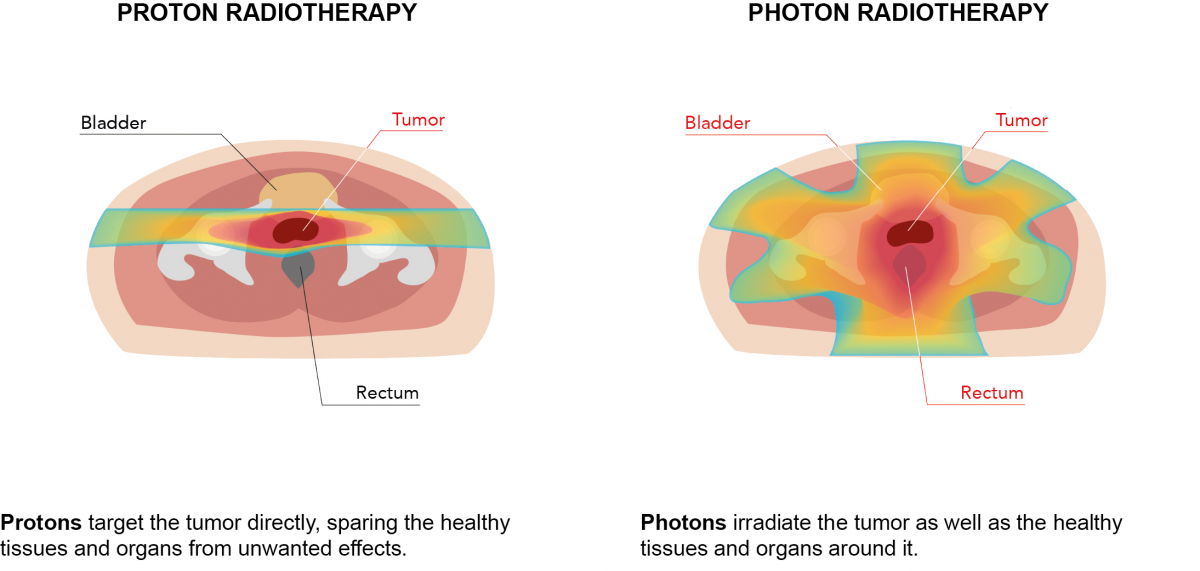
In the case of high-risk prostate carcinoma, proton radiotherapy allows for irradiation of the pelvic lymph nodes with high probability of subclinical affection. This clinical situation best reflects the dosimetric and clinical benefits of proton radiotherapy as it causes no harm to organs in the abdominal cavity, in particular intestinal villi.
Proton radiotherapy is a fully outpatient therapy. For low- and moderate-risk prostate carcinoma, it is possible to use stereotactic radiation lasting 10 days.
According to current international guidelines, both methods (photon and proton radiation) are considered applicable. Proton therapy is not a new method. Since 1991, the first exclusively clinical (not academic) workplace located at Loma Linda University, California, USA has treated many tens of thousands of patients diagnosed with prostate cancer using proton therapy. Proton therapy is a technologically mature treatment proven by almost three decades of clinical operation. Over the past two years, there have been many publications describing the results and advantages of protons for a given diagnosis.
Excellent long-term results are available from major prospective studies and data supporting proton therapy’s higher effectiveness and safety in comparison with photon radiation (IMRT). The data come mainly from the USA and Japan, i.e. from countries where proton radiotherapy has the strongest supportive environment (for example, in the USA there are already 26 centres, with 9 nearing completion) and is seen as a common procedure. In 2018, convincing data and published papers were reflected in the updated recommendations of the American Society for Therapeutic Radiology and Oncology according to whose current guidelines (NCCN Guidelines v. 4 2018) proton radiotherapy of prostate carcinoma is considered a standard therapeutic method for prostate carcinoma.
In 2016, a major randomised study was published in the New England Journal of Medicine evaluating the effectiveness of treatment and the quality of life of prostate carcinoma patients treated surgically, by radiotherapy or initially only actively monitored. The study was conducted in 1,643 patients and the follow-up period was 10 years. The study demonstrated that:
- mortality from prostate carcinoma does not differ between individual groups, and no difference in deaths from any causes was proven;
- in patients treated by surgery or radiation therapy, there was a lower risk of disease progression and metastatic disease development;
- radiotherapy had a temporary negative impact on sexual functions with subsequent improvements and did not affect urinary incontinence. Gastrointestinal symptoms were observed after radiotherapy for 6 months with subsequent improvements, whereas they were not observed in other modalities;
- from the viewpoint of quality of life, the trial showed that surgical treatment has the worst results in terms of sexual functions and urinary incontinence, and even though certain improvements were observed after some time, the results of surgical treatment remained the worst in these areas throughout the duration of the clinical study.